Article Text

Abstract
The impact of flavonoids on fatigue has not been investigated in relapsing and remitting multiple sclerosis (RRMS).
Objective To determine the feasibility and estimate the potential effect of flavonoid-rich cocoa on fatigue and fatigability in RRMS.
Methods A randomised double-blind placebo-controlled feasibility study in people recently diagnosed with RRMS and fatigue, throughout the Thames Valley, UK (ISRCTN69897291). During a 6-week intervention participants consumed a high or low flavonoid cocoa beverage daily. Fatigue and fatigability were measured at three visits (weeks 0, 3 and 6). Feasibility and fidelity were assessed through recruitment and retention, adherence and a process evaluation.
Results 40 people with multiple sclerosis (10 men, 30 women, age 44±10 years) were randomised and allocated to high (n=19) or low (n=21) flavonoid groups and included in analysis. Missing data were <20% and adherence to intervention of allocated individuals was >75%. There was a small effect on fatigue (Neuro-QoL: effect size (ES) 0.04, 95% CI −0.40 to 0.48) and a moderate effect on fatigability (6 min walk test: ES 0.45, 95% CI −0.18 to 1.07). There were seven adverse events (four control, three intervention), only one of which was possibly related and it was resolved.
Conclusion A flavonoid beverage demonstrates the potential to improve fatigue and fatigability in RRMS.
- fatigue
- cocoa
- diet
- multiple sclerosis
- flavonoids
Statistics from Altmetric.com
Introduction
Ninety per cent of people with multiple sclerosis (pwMS) experience fatigue.1 Fatigue and fatigability are difficult to treat and greatly affect health related quality of life in pwMS.2 Fatigability is a term derived from the broader definition of fatigue which refers to an inability to maintain both physical and cognitive performance.3 The aetiology of fatigue in MS is complex and includes possible neural, inflammatory, metabolic and psychological mechanisms.2 4 While several behavioural and drug approaches for fatigue management have been explored, to date the strongest evidence of success in reducing MS related fatigue is from exercise interventions.5 6 However, success is limited and other approaches or combination therapies need to be investigated.7
Dark chocolate containing 70–85% cocoa solids is well known for its high antioxidant and flavonoid content. Over a 4-week period, dark chocolate consumption has been shown to improve subjective fatigue in those with chronic fatigue syndrome (CFS),8 9 and results from a small randomised controlled pilot study using a short-term cocoa intervention suggested an increase in sleep quality and reduction in fatigue.10 A simple dietary supplement could be implemented alongside other behavioural interventions early after diagnosis as an adjunctive therapeutic approach to support pwMS to manage fatigue. There is currently limited evidence-based guidance to inform tailored dietary advice for symptom management in pwMS. Most diet based studies to date have looked at the risk of development or relapses in MS.11 12 However, modifiable lifestyle factors strongly correlate with clinically significant fatigue and remain a target for therapeutic trials.13 To date there has been limited research assessing the effect of dietary interventions in pwMS,14 but they have identified good adherence to dietary interventions.
We propose that a flavonoid approach for managing MS related fatigue may be moderately effective, inexpensive and safe,15 and that it may be exerting its effects by reducing inflammation and oxidative stress. The aim of the current trial was to evaluate the feasibility and estimate the potential effect to inform a follow-on substantive trial. The following key objectives were assessed: (1) the acceptance of the study design and diet intervention by participants; (2) monitoring recruitment rate and the process of randomisation, adherence to the protocol and loss to follow-up; (3) efficiency of data collection methods; (4) the estimate of effect size for fatigue, fatigability and other measures.
Methods
This was a parallel, randomised double-blind placebo-controlled trial to assess feasibility and efficacy (trial registration ISRCTN69897291; ethical approval National Research Ethics Service (Solihull, West Midlands) reference: 199515). Oxford Brookes University acted as sponsor and the study was conducted in accordance with the Declaration of Helsinki.
Recruitment
Recruitment was through neurology clinics in the Thames Valley, UK. In addition, local MS Society branches were made aware of the trial and given contact details, and an advertisement for the study along with the participant information sheet was made available on the MS Society website. Individuals were able to self-refer to the study by contacting the researchers.
Setting
The intervention took place in the home of each participant. All testing took place at Oxford Brookes University, Oxford, UK except for optional home visits at week 3. Assessments took place between 07:30 and 10:00 and the intervention lasted a total of 6 weeks with three testing visits (baseline, week 3 and week 6).
Randomisation and allocation
After recruitment, participants were allocated the next available study number by the blinded assessor. The study number related to a computer-generated randomisation list held by the principle investigator and randomised individuals (1:1) into the intervention group or the control group. The randomisation list used minimisation to balance groups for gender and whether individuals were on disease modifying treatments (DMTs) at baseline. The list provided a three digit code that related to a code on identical pre-package sachets (made up by a co-investigator) containing either intervention or control cocoa. The sachets were then dispensed to the participant. The intervention began 3 days after baseline. Group allocation was concealed throughout the study and analysis.
Eligibility
Eligibility criteria were: adults aged ≥18 years with a <10 year clinical diagnosis of relapsing and remitting multiple sclerosis, either treatment naïve or taking first line DMTs (online supplementary file 1); no relapse or sudden change in MS symptoms within the previous 3 months; no contraindications to providing a blood sample or tolerating the cocoa drink; fatigue greater than 4 out of 7 on the Fatigue Severity Scale (FSS)16; no other conditions that may be associated with fatigue (eg, anaemia); not on medication for the treatment of depression; an Expanded Disability Status Scale (EDSS) score <4.517; sufficient mental capacity to consent; able to walk with or without a walker for at least 16 m; no condition affecting the central nervous system other than MS (migraine and headache were allowed); not pregnant or lactating; and no objection to the researchers contacting their general practitioner (family doctor) and neurologist.
Supplemental material
Intervention
Participants were provided with cocoa by the lead researcher at baseline and at week 3, and they were asked to consume the drink in their homes daily. Cocoa was consumed after an overnight fast at the same time each morning. After the consumption of the drink, they were instructed to wait 30 min before consuming any other food or beverage and/or take their medication. Participants were instructed to take their medication and to follow their usual diet for the rest of the day. The cocoa drinks (intervention and control) were designed to differ only in flavonoid content (low vs high flavonoid; online supplementary file 2). Cocoa powder was provided to participants in air tight individual sachets. They were asked to add the sachet content to a mug and to add heated rice milk before consuming the drink. Instructions on preparation were provided to ensure all participants followed the same protocol. Unused cocoa powder was collected by the researcher at the next assessment.
Supplemental material
Outcomes
The primary aim was to assess the feasibility of the dietary intervention in terms of recruitment rate and the process of randomisation, adherence to the protocol and loss to follow-up, safety and process. We documented adverse events (AEs). Duration of participation and dropout from the intervention were also recorded. Appropriateness of data collection methods was determined through completion of questionnaires and missing data, and through the process evaluation, and estimates of effect (effect sizes (ES) and 95% confidence intervals (95% CI)) were calculated for the measures and the demographics were collected at baseline.
Fatigue and fatigability
Throughout the 6-week intervention participants were asked to rate their level of fatigue on a numerical rating scale (NRS) through daily ‘fatigue texts’ rating their fatigue between 1–10 (10 worst). They replied to the text message of “on a scale from 1 to 10, with one being no fatigue and 10 being the worst fatigue you have experienced, how fatigued are you at the current time?”. They did this at 10:00, 15:00 and 20:00 every day for 6 weeks. Fatigability was measured at baseline and week 6 using the 6 min walk test (6MWT).18 Participants were asked to walk at their normal, comfortable walking pace back and forth on a measured 16 m track in a university corridor. Distance walked was measured. At baseline, week 3 and week 6 the levels of subjective fatigue experienced over the past 7 days were measured using the Neuro-QOL short form questionnaire.19 The Adult Memory and Information Processing Battery (AMIPB)20 was used to measure cognitive fatigue. The AMIPB required the second highest number in each row to be circled, with 15 rows of five double digit numbers. Participants had 2 min and their attempts were timed, with incorrect answers being noted.
Questionnaires administered at baseline, week 3 and week 6 were: the Physical Activity Scale for the Elderly (PASE),21 EQ5D-5L,22 Preference-Based Multiple Sclerosis Index (PBMSI)23 and the Hospital Anxiety and Depression Scale (HADS).24 Demographic information was collected. A previously published protocol paper gives detail about each measure.25 Activity was monitored with 7-day wrist worn accelerometers (Axivities) before, and over two separate weeks of the trial (week 2–3 and week 5–6).
Blood markers of inflammation were measured, including tumour necrosis factor α (TNFα), reduced glutathione, a marker of antioxidant status and lipid peroxidation.
A detailed description of the measures can be found in online supplementary file 1.
Process evaluation
On exiting the study at week 6, each participant was interviewed about the intervention process, ease of adherence, tolerance and acceptability of the flavonoid drink, and the collection of outcome measures. Participants were asked their opinion on the importance of the research question proposed to inform future trials. The 13 topics used included difficulties with intervention delivery, scheduling of assessments and outcome measure acceptability, and suggestions on how to improve the intervention process. A proportion of the data (20%) was coded by two different team members to check on reliability of the coding scheme. Transcripts of interviews were examined to identify themes and categories. Codes were applied to these broad themes, which were then broken down further into sub-codes. Agreement on concepts and coding by blinded assessors were sought between two members of the research team to ensure reliability.
Analysis
Feasibility was analysed through evaluation of eligibility, recruitment and retention.26 Completeness of outcome measures was reported and 80% was set as a criterion for success. Retention was measured by the proportion of participants who were lost to follow-up. Successful adherence to the intervention was defined as at least 75% of the participants having completed cocoa consumption. Further aspects of adherence were measured by the percentage of fatigue texts completed by participants.
Primary analysis followed the intention to treat principal and utilised the complete case dataset. Results were presented using point estimates and 95% CI. For the fatigue texts the fatigue NRS was calculated as the area under the curve (AUC) for each group, ignoring the area beneath the baseline, and was calculated geometrically.27 Data were transformed to improve model fit, or different regression approaches were used (eg, negative binomial, or Poisson regression). The results for the 6MWT are reported as mean±SD and for the comparison of baseline and post-intervention as mean difference±standard error (SE, 95% CI). A linear mixed model (LMM) was used to detect differences between groups throughout all time points. Alternatively and wherever the variables were categorical, such as the EQ5D-5L sub categories, a generalised estimating equation (GEE) with appropriate distributions (eg, negative binomial) method was implemented. Both methods used SAS/STAT 14.3. Fatigue and fatigability measures including the Neuro-QoL short form fatigue, the 6MWT and the AMIPB were further analysed to determine the difference between responders and non-responders and relative risk scores were then calculated. Responders on the NeuroQol, for both the control and intervention groups, were classified as those who had a clinically meaningful change of 10 points out of 100 (with the questionnaire total score converted from an original total of 40 between baseline and week 6). Responders on the 6MWT were classified as those who had a minimally important change (MIC) in covered distance of 21.6 m27 between baseline and week 6.
Data over three time points for activity data were analysed using a Freidman’s test and between group effects were calculated using a Mann-Witney test. Process evaluation included frequencies for adhering to the intervention, session content and progression which was analysed descriptively with confidence intervals and regression where possible. Standard content analysis techniques were employed.
Results
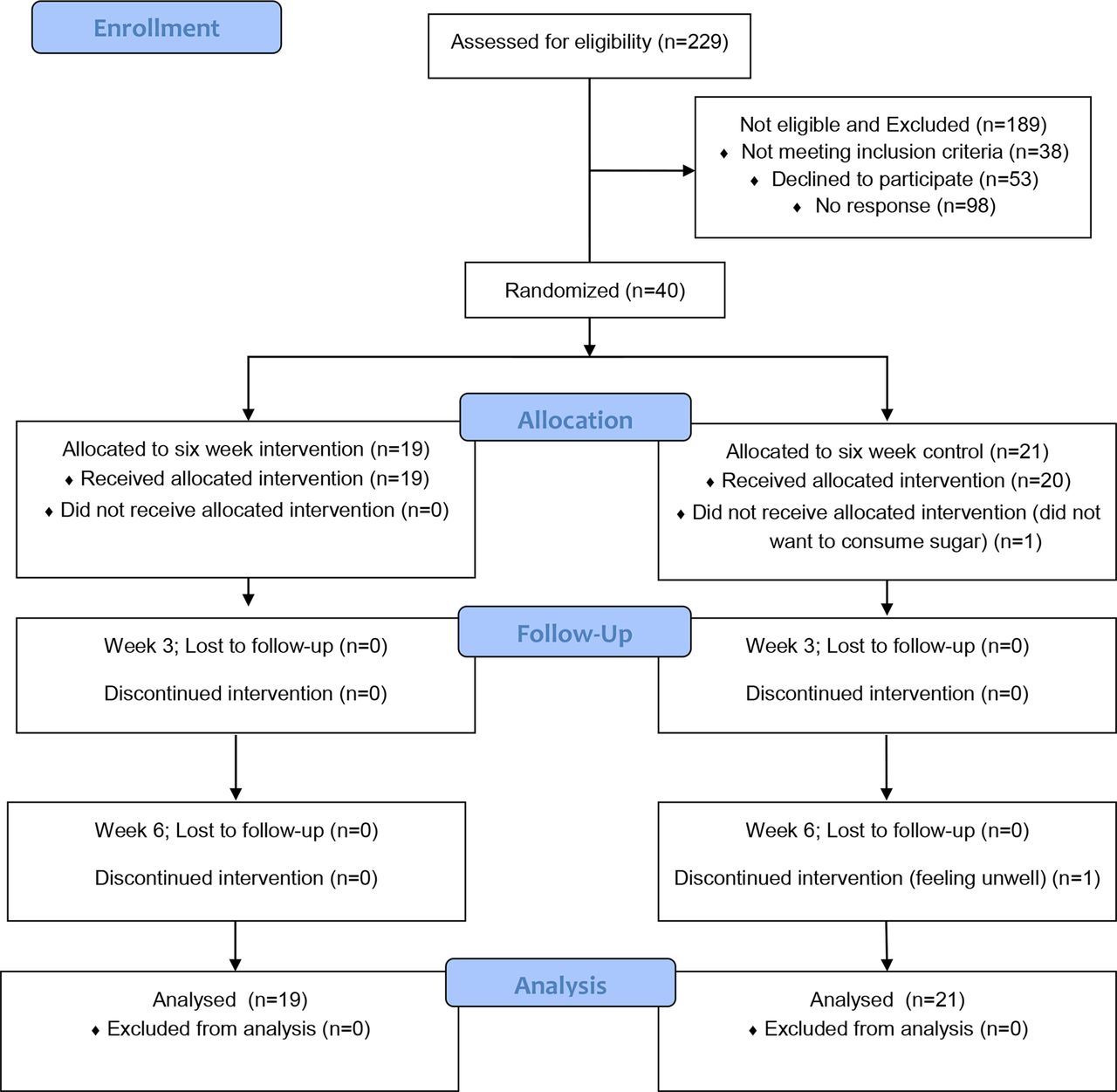
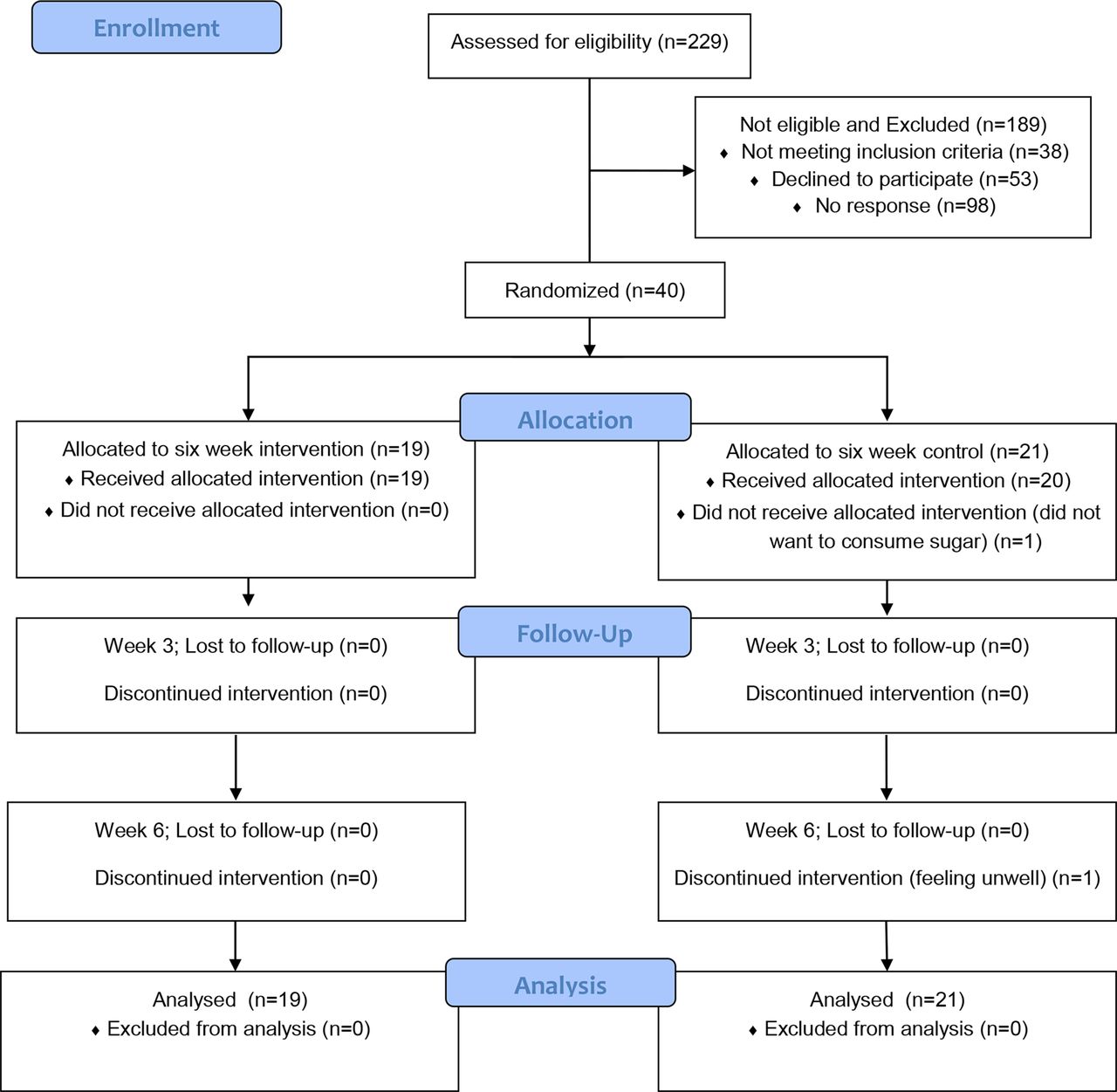
Between May 2016 and August 2017, 40 pwMS were recruited from four neurology clinics, including Oxford University Hospitals NHS Trust (John Radcliffe Hospital site), Milton Keynes hospital, Royal Berkshire hospital or Buckingham hospital, or through advertisements and online media (MS Society webpage and MS Trust Facebook page).
Figure 1 shows the participant flow. It was not possible to determine the total number of people screened.
{kind=link}
Flow of recruitment: the screening and enrolment process for a 6-week randomised double-blind placebo-controlled feasibility trial in people with multiple sclerosis. A total of 40 people were included in the final analysis, and reasons for not receiving the allocated intervention (cocoa drink) and discontinuation are presented.
Feasibility
Fifty-three people showed an initial interest in the trial, but decided not to take part due to not having enough time to take part in the trial, did not like chocolate, or were unable to take part in nutrition trials due to being on a weight loss programme or having gastric surgery. All but one person consumed the cocoa with rice milk (one consumed almond milk). One person discontinued the control intervention but was not lost to follow-up and one person consented to be on the trial but decided not to consume the cocoa from the start of the intervention. Adherence to intervention overall was 100% (19/19) for the intervention group and 90% (19/21) for the control group. Missing data from NRS was <20% of total responses, but reporting did drop in week 6. Blood measures were only achieved in 20 participants (after a maximum of three attempts). Overall missing data for secondary measures were <20%. There were seven AEs during the trial, caused by worsening fatigue, feelings of nausea, or a general feeling of being unwell. AEs were considered unlikely to be related (five), possibly related but expected/resolved (one), and not related to the intervention (one). Four AEs were associated with the control cocoa and three with the high flavonoid cocoa. There were no incidences of un-blinding of the researcher or participant. Five out of 40 people were seen at home at week 3.
Demographic and clinical data are shown in table 1. There were no significant differences for demographics between the groups at baseline (p>0.05).
Demographic information at baseline for both groups
Outcome measures
Between group effect sizes were considered from all three assessments points. Efficacy potential of fatigue and feasibility was determined. A breakdown of the outcome measures is shown in table 2.
Results for outcome measures at baseline, week 3 and week 6 of the intervention*
Physical activity levels over the intervention period can be seen in table 3.
Physical activity levels (reported in minutes per day on average) using an accelerometer watch before the intervention, between 9 to 16 days (3 weeks) into the intervention, and between 35 to 42 days (6 weeks) at the end of the intervention, broken down into sedentary, light, moderate and vigorous classification
Fatigue and fatigability
Fatigue was further analysed to determine the difference between responders and non-responders. There was no difference in means between groups (p>0.05) yet the relative risk for those who responded and therefore had improved fatigue in the intervention group (11 out of 19 responders) compared to the control group (8 out of 20 responders) was 1.45. The AMIPB was assessed in a similar way with a change in 1 SD of an improvement in 11.5 s considered clinically meaningful. Based on these criteria only one person improved in the intervention group and no one in the control group, and therefore a relative risk was not calculated.
There was a medium effect size for distance walked in 6 min (0.45, 95% CI 0.18 to 1.07) between the groups with the intervention showing a larger increase in the metres walked in 6 min after the intervention (table 2). The relative risk for responders in the intervention group compared with the control group was 1.80 in favour of the intervention group.
Process evaluation
Both groups had similar positive experiences about the scheduling of the assessments. Thirteen of 19 in the intervention group versus 18/20 people in the control group indicated no impact of the measurement instruments used on weekly routine over the 6 weeks. Similar numbers in both groups identified that the outcome measures were acceptable. Randomisation: Most comments from both groups indicated acceptance towards the process of randomisation. Taste: Similar numbers (8/19 intervention vs 9/20 control) reported positive comments about the taste of the cocoa. Procedures and routine of preparing the drink: A few individuals in both groups identified that it was inconvenient to wait for food after drink consumption (4/19 intervention vs 3/20 control), and that the process did not always fit in with their lifestyle, for example, travelling. Other individuals (15/19 intervention vs 17/20 control) identified that they worked it into a routine. Continuation of consuming the drink: half of both groups (9/19 intervention vs 11/20 control) said they would continue the drink if offered. A further four people in both groups said they would continue if it was beneficial or if they could implement their own routine.
Discussion
PwMS engaged with the dietary intervention, with fatigue and fatigability measures responding more in the intervention group with effect sizes calculated. The current study was shown to be feasible and well received by pwMS, with high adherence to the intervention and excellent data completion. Our study establishes that the use of dietary interventions is feasible and may offer possible long-term benefits to support fatigue management, by improving fatigue and walking endurance. We further propose that considering the possible anti-inflammatory mechanism, flavonoids may be used as an adjunctive approach alongside other therapeutic interventions and suggest the possible benefit of such combined approaches for fatigue management. However further full powered trials would need to be performed.
The time post diagnosis was extended from 5 to 10 years in order to recruit to target (n=40). Adherence (>75%), retention and amount of missing data (<80%) were within the acceptable ranges. Most missing data were from the NRS texts over the 6 weeks which is not surprising as this was the most time-consuming part of the assessment. Completion was still above 80% of total with the first 5 weeks, with week 6 showing the most missing data. Mild AEs have previously been reported when consuming high flavonoid cocoa and include nausea and vomiting, gastrointestinal disturbances and headaches.28 The AEs reported in the current trial did not cause any safety concerns and were similar between groups.
This is the first study to suggest the potential for fatigability can be improved through a 6MWT after 6 weeks of a flavonoid intervention, with a moderate effect size. In the current study the intervention showed an MIC over time with 33.7 m (SE 8.4) in contrast to the control group 10.2 m (SE 9.6). Fatigue correlates with a decrease of physical endurance29 and walking speed30 and therefore a treatment targeting fatigue could also improve walking performance. Flavonoids have been found to increase cerebral blood flow by inducing widespread stimulation of brain perfusion, and this could also influence mood, cognitive performance, fatigue perception and ability to perform specific movement tasks.31 When considering other symptoms, pain was shown to improve in the flavonoid group over the 6 weeks as measured by the EQ5D-5L with a moderate effect size. The antioxidant properties of flavonoids are thought to lessen neuropathic pain by alleviating oxidative stress and thus reducing neuron damage caused by lipid peroxidation.32 We did not measure objective measures of pain in this trial and therefore further research is warranted to explore the pain improvement. Indeed previous research has pointed towards higher motivation in physical activity in pwMS when symptoms such as pain were improved.33 This may also allow pwMS to become more active and mobile, as noted by the improvements on the 6MWT.
The process evaluation revealed that overall the trial was well accepted, with the timing of assessments and the outcome measures being convenient and a low burden, respectively, and the participants in both groups found the taste of the cocoa enjoyable, or noted it as neither tasty nor unacceptable. In both groups the blinding and randomisation processes were accepted, and a majority of pwMS in both groups declared their willingness to continue consuming the cocoa long term, especially if benefits for fatigue were found. However, findings around the preparation of the drink and/or scheduling the timing of drink consumption into one’s routine are factors to consider for future trials.
Limitations
As a feasibility study a powered investigation using a sample size of 80 is now needed. For blood measures, the lack of ability of the phlebotomist to collect blood from several of the participants led to missing data. From the data collected, there were small effect sizes in blood indicators, apart from lipid peroxidation which showed a moderate effect size and therefore this area needs further investigation. The NRS fatigue data were analysed as a total whole change over the 6 weeks, and therefore more sensitive analysis may have discovered changes within the 6 weeks. Fatigue may be both physical and cognitive and coexists with, and is impacted by, a number of factors including anxiety and depression. This study measured a number of these factors, including motor (6MWT) and cognitive (AMIPB) fatigue, and anxiety and depression (HADS), which could be further investigated in a study powered for this. In this pilot we set out to reduce variability from these factors where possible; for example, we excluded individuals with a clinical diagnosis or receiving treatment for depression (such as individuals on antidepressants).
It should be considered that, while we used a wide range of recruitment methods, thus reducing the risk of recruitment bias, participants were recruited from affluent areas of the UK. Acknowledging this limitation, we nevertheless propose the responses in outcome measures are largely generalisable to relatively healthy pwMS.
Conclusion
The use of dietary approaches to reduce fatigue and associated factors in pwMS may be an easy, safe and cost effective way to have an impact on quality of life and independence, allowing people to feel more in control of their condition. A full evaluation including wider geography, longer follow-up and cost effectiveness is now indicated. This technology has the potential to be implemented in the UK and worldwide, alongside other rehabilitation measures including exercise, DMTs and physiotherapy.
References
Supplementary materials
Press release
Footnotes
Contributors SC, JC, AS, MC, AC, STW, JP, GD, JMH, EB and HD were involved in the design and ongoing conduct of the project. SC and HD were responsible for the overall conduct of the project. JC, JC, AS, LD, MK, and HD were responsible for the data collection and day to day running of the trial. HI was involved in the stastical analysis of the project. All authors were involved in the writing and proof reading of the project. Wade was responsible for AEs.
Funding Funding for the trial was granted from the Multiple Sclerosis Society; Grant reference 32. HD is funded by Elizabeth Casson Trust and Higher Education Thames Valley and the Biomedical Research Centres. JC is funded by Heath Education Thames Valley. Disclosure funding for highly specialised services to run a national congenital myasthenia service and a neuromyelitis service. Support for scientific meetings and honorariums for advisory work from Merck Serono, Biogen Idec, Novartis, Teva, Abide, Chugai Pharma, Alexion, MedDay, Argenx and Bayer Schering, Medimmune and unrestricted grants from Merck Serono, Novartis, Biogen Idec, Chugai, Alexion and Bayer Schering. MS society and Guthie Jackson Foundation research grants.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval was granted from the National Research Ethics Service {Solihull West Midlands reference: 199515).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial commentary