Effectiveness of a Serious Game for Cognitive Training in Chronic Stroke Survivors with Mild-to-Moderate Cognitive Impairment: A Pilot Randomized Controlled Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Neuro-World Games
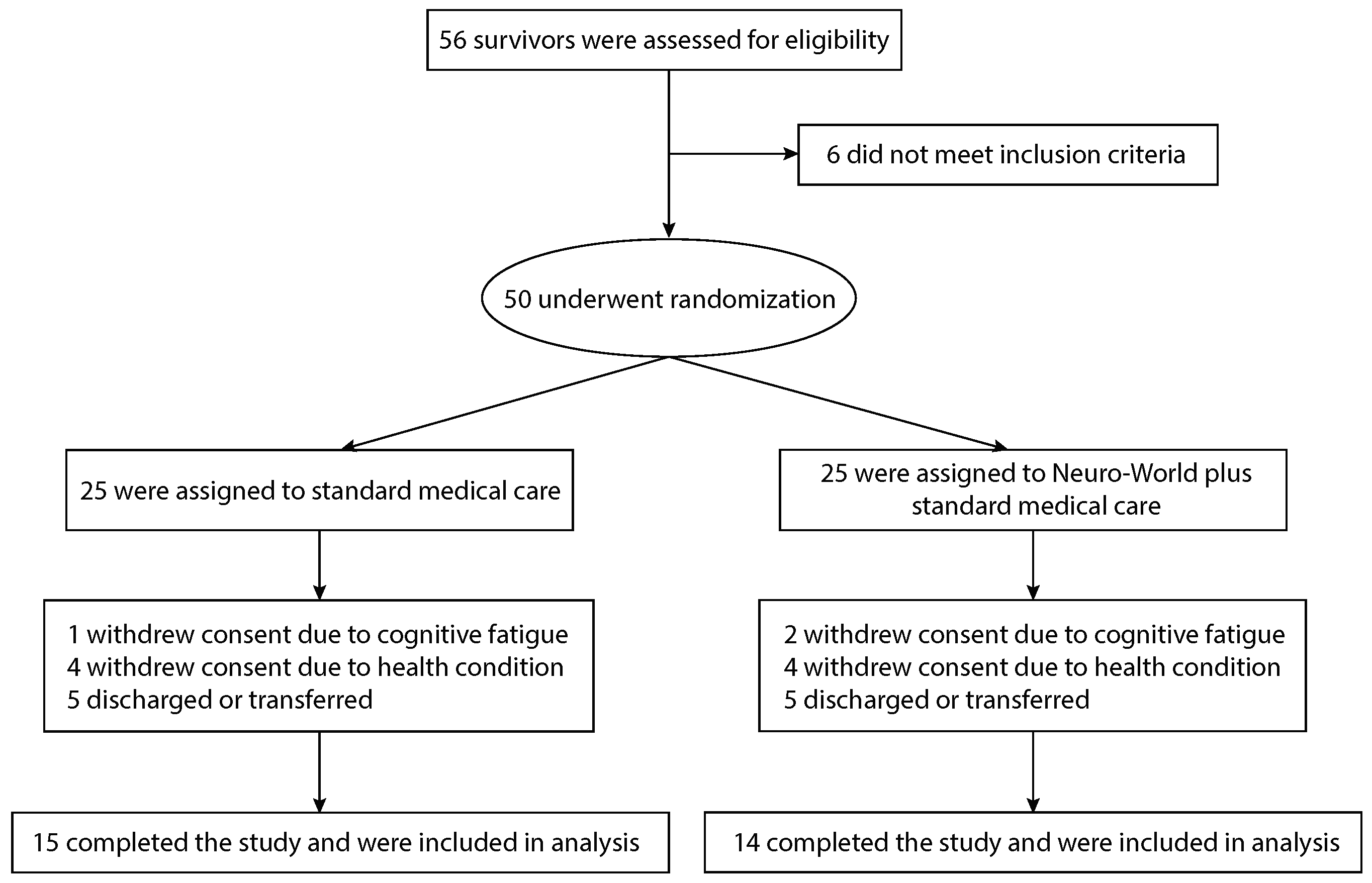
2.2. Study Design and Enrollment
2.3. Outcome Measures
2.3.1. Primary Outcome
2.3.2. Secondary Outcomes
2.4. Statistical Analyses
3. Results
3.1. Study Population
3.2. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Neuro-World Games

{kind=link}
{kind=link}
{kind=link}
| Game | Mechanics of Difficulty Adjustment |
|---|---|
| 1 | One animal enters and leaves the farm in stage one whereas, in stage 20, ten animals enter and five of them leave. The speed of all the animals in stage 20 move 2.1 times faster than the speed in stage one when entering and leaving the farm. |
| 2 | One animal enters and leaves the farm in stage one whereas, in stage 20, ten animals enter and four of them leave the farm. |
| 3 | Three animals enter and all three animals remain on the farm in stage one. In stage 20, 16 animals enter and 12 of them remain on the farm. The speed of all the animals in stage 20 move 3.2 times faster than the speed in stage one when entering and leaving the farm. |
| 4 | A total of four animals are presented while 40 animals are presented in stage 20. In stage one, each type of animal has only one color whereas, in stage 20, each type of animal has multiple skin colors. |
| 5 | Two animals are presented in stage one whereas nine animals are presented in stage 20. |
| 6 | Only one shape is used to make a sequence in stage one whereas 15 different combinations of primitive shapes are used in stage 20. The sequence presented at the bottom of the screen consists of seven (identical) shapes in stage one and 14 shapes (using different combinations of primitive shapes) in stage 20. |
Appendix B. Neuro-World Games
| Gameplay Data | Game 1 | Game 2 | Game 3 | Game 4 | Game 5 | Game 6 |
|---|---|---|---|---|---|---|
| Highest mean (std) stage | 20 (0) | 18 (3) | 6 (2) | 20 (0) | 13 (3) | 20 (1) |
| Gameplay mean (std) count | 18 (4) | 9 (1) | 4 (1) | 11 (2) | 47 (14) | 5 (1) |
| Time for each gameplay, mean (std) seconds | 17 (4) | 37 (3) | 100 (46) | 30 (7) | 7 (2) | 50 (67) |
| Rate of correct answer, mean (std) % | 70 (19) | 45 (16) | 42 (19) | 68 (18) | 60 (21) | 60 (19) |
Appendix C. Study Population
| ID | Age | Sex | Diagnosis | Chronicity | Affected Side | MFT (Lt/Rt) | Location of Stroke | Handedness |
|---|---|---|---|---|---|---|---|---|
| 1 | 66 | F | Isc | 156 | Lt | 5/23 | N/A | Rt |
| 2 | 81 | F | Isc | 121 | Rt | 27/22 | N/A | Rt |
| 3 | 62 | F | Isc | 108 | Lt | 2/28 | MCA Inf | Rt |
| 4 | 71 | F | Isc & Alz | 78 | Lt | 0/28 | N/A | Rt |
| 5 | 85 | F | Isc | 38 | Lt | 22/27 | N/A | Rt |
| 6 | 72 | F | Isc | 54 | Rt | 29/25 | N/A | Rt |
| 7 | 80 | M | Hem | 64 | Lt | 23/24 | T SDH | Rt |
| 8 | 75 | F | Isc | 76 | Rt | 29/22 | N/A | Rt |
| 9 | 77 | F | Isc | 41 | Rt | 28/10 | Lt MCA Inf | Lt |
| 10 | 64 | F | Hem | 132 | Lt | 7/31 | N/A | Rt |
| 11 | 85 | F | Isc | 24 | Rt | 26/21 | N/A | Rt |
| 12 | 50 | M | Hem | 72 | Rt | 29/10 | Lt FPT SDH | Rt |
| 13 | 70 | F | Isc | 35 | Rt | 23/2 | Rt BG, IC Inf | Rt |
| 14 | 80 | F | Isc | 38 | Lt | 25/27 | Lt BG Inf | Rt |
| ID | Age | Sex | Diagnosis | Chronicity | Affected Side | MFT (Lt/Rt) | Location of Stroke | Handedness |
|---|---|---|---|---|---|---|---|---|
| 1 | 81 | F | Isc | 58 | Lt | 22/26 | Rt ACA Inf | Rt |
| 2 | 87 | F | Isc | 36 | Lt | 9/25 | Rt MCA Inf | Rt |
| 3 | 76 | F | Isc | 53 | Rt | 29/11 | N/A | Rt |
| 4 | 87 | F | Isc | 70 | Lt | 19/25 | N/A | Rt |
| 5 | 77 | F | Isc | 40 | Rt | 29/4 | BG Inf w/ HT | Rt |
| 6 | 87 | F | Isc | 64 | Rt | 28/17 | N/A | Rt |
| 7 | 49 | F | Isc | 24 | Rt | 30/13 | Lt TH | Rt |
| 8 | 66 | F | Hem | 68 | Rt | 31/26 | N/A | Rt |
| 9 | 56 | F | Isc | 48 | Lt | 8/29 | N/A | Rt |
| 10 | 80 | F | Isc | 37 | Rt | 29/24 | MCA, PCA Inf | Rt |
| 11 | 78 | F | Isc | 84 | GD | 30/31 | BL PVWM Inf | Rt |
| 12 | 73 | F | Isc | 28 | Rt | 30/23 | Lt TH Inf | Rt |
| 13 | 67 | M | Isc | 24 | Rt | 28/12 | N/A | Rt |
| 14 | 75 | F | Hem | 24 | Lt | 18/27 | O ICH | Rt |
| 15 | 50 | M | Isc | 24 | Rt | 28/11 | Rt BG Inf | Rt |
Appendix D. Secondary Cognitive Outcomes
| Outcomes | Intervention Experimental vs. Control | Time Baseline vs. Post-Intervention | Interaction Intervention×Time | |||
|---|---|---|---|---|---|---|
| Total MMSE | ||||||
| Orientation | ||||||
| Register | ||||||
| Attention & Calculation | ||||||
| Recall | ||||||
| Language | ||||||
| DFS | ||||||
| DBS | ||||||
| GDS | ||||||
| Outcomes | Experimental Baseline vs. Post-Intervention | Control Baseline vs. Post-Intervention | ||
|---|---|---|---|---|
| Total MMSE | ||||
| Orientation | ||||
| Register | ||||
| Attention & Calculation | ||||
| Recall | ||||
| Language | ||||
| DFS | ||||
| DBS | ||||
| GDS | ||||
| Outcomes | Baseline Experimental vs. Control | Post-Intervention Experimental vs. Control | ||
|---|---|---|---|---|
| p | (27) | p | ||
| Total MMSE | ||||
| Orientation | ||||
| Register | ||||
| Attention & Calculation | ||||
| Recall | ||||
| Language | ||||
| DFS | ||||
| DBS | ||||
| GDS | ||||
Appendix E. GDS Results and Implications
References
- Benjamin, E.J.; Muntner, P.; Bittencourt, M.S. Heart disease and stroke statistics-2019 update: A report from the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]
- Tatemichi, T.K.; Paik, M.; Bagiella, E.; Desmond, D.W.; Pirro, M.; Hanzawa, L.K. Dementia after stroke is a predictor of long-term survival. Stroke 1994, 25, 1915–1919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Middleton, L.E.; Lam, B.; Fahmi, H.; Black, S.E.; McIlroy, W.E.; Stuss, D.T.; Danells, C.; Ween, J.; Turner, G.R. Frequency of domain-specific cognitive impairment in sub-acute and chronic stroke. NeuroRehabilitation 2014, 34, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Cumming, T.B.; Marshall, R.S.; Lazar, R.M. Stroke, cognitive deficits, and rehabilitation: Still an incomplete picture. Stroke 2013, 8, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Leys, D.; Esquenazi, A. The interaction between neuropsychological and motor deficits in patients after stroke. J. Neurol. Neurosurg. Psychiatry 2013, 80, S27–S34. [Google Scholar] [CrossRef]
- Mullick, A.A.; Subramanian, S.K.; Levin, M.F. Emerging evidence of the association between cognitive deficits and arm motor recovery after stroke: A meta-analysis. Restor. Neurol. Neurosci. 2015, 33, 389–403. [Google Scholar] [CrossRef] [Green Version]
- Nakling, A.; Aarsland, D.; Næss, H.; Wollschlaeger, D.; Fladby, T.; Hofstad, H.; Wehling, E. Cognitive Deficits in Chronic Stroke Patients: Neuropsychological Assessment, Depression, and Self-Reports. Dement. Geriatr. Cogn. Disord. Extra 2017, 7, 283–296. [Google Scholar] [CrossRef]
- Montana, J.I.; Matamala-Gomez, M.; Maisto, M.; Mavrodiev, P.A.; Cavalera, C.M.; Diana, B.; Mantovani, F.; Realdon, O. The Benefits of emotion Regulation Interventions in Virtual Reality for the Improvement of Wellbeing in Adults and Older Adults: A Systematic Review. J. Clin. Med. 2020, 9, 500. [Google Scholar] [CrossRef] [Green Version]
- Pham, Q.; Khatib, Y.; Stansfeld, S.; Fox, S.; Green, T. Feasibility and efficacy of an mHealth game for managing anxiety:“flowy” randomized controlled pilot trial and design evaluation. Games Health J. 2016, 5, 50–67. [Google Scholar] [CrossRef]
- Pasquini, M.; Leys, D.; Rousseaux, M.; Pasquier, F.; Henon, H. Influence of cognitive impairment on the institutionalisation rate 3 years after a stroke. J. Neurol. Neurosurg. Psychiatry 2007, 78, 56–59. [Google Scholar] [CrossRef] [Green Version]
- Claesson, L.; Linden, T.; Skoog, I.; Blomstrand, C. Cognitive Impairment after Stroke–Impact on Activities of Daily Living and Costs of Care for Elderly People. The Goteborg 70+ Stroke Study. Cerebrovasc. Dis. 2005, 19, 102–109. [Google Scholar]
- Langhorne, P.; Baylan, S. Early supported discharge services for people with acute stroke. Cochrane Datab. Syst. Rev. 2007, 7, 1–25. [Google Scholar]
- Bassett, S.F. The assessment of patient adherence to physiotherapy rehabilitation. N. Z. J. Physiother. 2003, 31, 60–66. [Google Scholar]
- Kueider, A.M.; Parisi, J.M.; Rebok, A.L.G.G.W. Computerized Cognitive Training with Older Adults: A Systematic Review. PLoS ONE 2012, 7, e40588. [Google Scholar] [CrossRef] [Green Version]
- Bogdanova, Y.; Yee, M.K.; Ho, V.T.; Cicerone, K.D. Computerized Cognitive Rehabilitation of Attention and Executive Function in Acquired Brain Injury: A Systematic Review. J. Head Trauma Rehabil. 2016, 31, 419–433. [Google Scholar] [PubMed] [Green Version]
- Van de Ven, R.M.; Murre, J.M.; Veltan, D.J.; Schmand, B.A. Computer-Based Cognitive Training for Executive Functions after Stroke: A Systematic Review. Front. Hum. Neurosci. 2016, 10, 150. [Google Scholar]
- Wentink, M.M.; Meesters, J.; Berger, M.A.M.; de Kloet, A.J.; Stevens, E.; Band, G.P.H.; Kromme, C.H.; Wolterbeek, R.; Goossens, P.H.; Vliet Vlieland, T.P.M. Adherence of stroke patients with an online brain training program: The role of health professionals’ support. Top. Stroke Rehabil. 2018, 25, 359–365. [Google Scholar] [PubMed]
- Anguera, J.A.; Boccanfuso, J.; Rintoul, J.L.; Al-Hashimi, O.; Faraji, F.; Janowich, J.; Kong, E.; Larraburo, Y.; Rolle, C.; Johnston, E.; et al. Video game training enhances cognitive control in older adults. Nature 2013, 501, 97–101. [Google Scholar]
- Thapa, N.; Park, H.J.; Yang, J.G.; Son, H.; Jang, M.; Lee, J.; Kang, S.W.; Park, K.W.; Park, H. The Effect of a Virtual Reality-Based Intervention Program on Cognition in Older Adults with Mild Cognitive Impairment: A Randomized Control Trial. J. Clin. Med. 2020, 9, 1283. [Google Scholar]
- Manera, V.; Ben-Sadoun, G.; Aalbers, T.; Agopyan, H.; Askenazy, F.; Benoit, M.; Bensamoun, D.; Bourgeois, J.; Bredin, J.; Bremond, C.J.C.; et al. Recommendations for the use of serious games in neurodegenerative disorders: 2016 Delphi Panel. Front. Psychol. 2017, 8, 1243. [Google Scholar]
- Mosimann, U.; Tarnanas, I.; Dimitriadis, S.; Laskaris, N.; Bamidis, P.; Tsolaki, M.; Nef, T.; Mueri, R.; Mosimann, U. P4-365: Serious Gaming Enhances Cognitive Function in Mci Due To Alzheimer’s Disease. Alzheimer Dement. 2014, 10, P922. [Google Scholar] [CrossRef]
- Michael, D.R.; Chen, S.L. Serious Games: Games That Educate, Train, and Inform; Course Technology PTR: Boston, MA, USA, 2005. [Google Scholar]
- Zyda, M. From visual simulation to virtual reality to games. Computer 2005, 38, 25–32. [Google Scholar] [CrossRef]
- Manera, V.; Petit, P.D.; Derreumaux, A.; Orvieto, I.; Romagnoli, M.; Lyttle, G.; David, R.; Robert, P.H. ‘Kitchen and cooking’ a serious game for mild cognitive impairment and Alzheimer’s disease: A pilot study. Front. Aging Neurosci. 2015, 7, 24. [Google Scholar] [CrossRef]
- Robert, P.; König, A.; Amieva, H.; Andrieu, S.; Bremond, F.; Bullock, R.; Ceccaldi, M.; Dubois, B.; Gauthier, S.; Kenigsberg, P.A.; et al. Recommendations for the use of Serious Games in people with Alzheimer’s Disease, related disorders and frailty. Front. Aging Neurosci. 2014, 6, 54. [Google Scholar] [CrossRef] [PubMed]
- Muscio, C.; Tiraboschi, P.; Guerra, U.P.; Defanti, C.A.; Frisoni, G.B. Clinical trial design of serious gaming in mild cognitive impairment. Front. Aging Neurosci. 2015, 7, 26. [Google Scholar] [CrossRef] [Green Version]
- Zickefoose, S.; Hux, K.; Brown, J.; Wulf, K. Let the games begin: A preliminary study using Attention Process Training-3 and LumosityTM brain games to remediate attention deficits following traumatic brain injury. Brain Inj. 2013, 27, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Radomski, M.V. More than good intentions: Advancing adherence to therapy recommendations. Am. J. Occup. Ther. 2011, 65, 471–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danzl, M.M.; Etter, N.M.; Andreatta, R.D.; Kitzman, P.H. Facilitating neurorehabilitation through principles of engagement. J. Allied Health 2012, 41, 35–41. [Google Scholar]
- Benyon, D.; Turner, P.; Turner, S. Designing Interactive Systems: People, Activities, Contexts, Technologies; Pearson Education: Upper Saddle River, NJ, USA, 2005. [Google Scholar]
- Westerberg, H.; Jacobaeus, H.; Hirvikoski, T.; Clevberger, P.; Östensson, M.; Bartfai, A.; Klingberg, T. Computerized working memory training after stroke—A pilot study. Brain Inj. 2007, 21, 21–29. [Google Scholar] [CrossRef]
- Lundqvist, A.; Grundström, K.; Samuelsson, K.; Rönnberg, J. Computerized training of working memory in a group of patients suffering from acquired brain injury. Brain Inj. 2010, 24, 1173–1183. [Google Scholar] [CrossRef]
- Hellgren, L.; Samuelsson, K.; Lundqvist, A.; Börsbo, B. Computerized Training of Working Memory for Patients with Acquired Brain Injury. Open J. Ther. Rehabil. 2015, 3, 46–55. [Google Scholar] [CrossRef] [Green Version]
- Mödden, C.; Behrens, M.; Damke, I.; Eilers, N.; Kastrup, A.; Hildebrandt, H. A Randomized Controlled Trial Comparing 2 Interventions for Visual Field Loss With Standard Occupational Therapy During Inpatient Stroke Rehabilitation. Neurorehabilit. Neural Repair 2012, 26, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Yoo, C.; Yong, M.; Chung, J.; Yang, Y. Effect of computerized cognitive rehabilitation program on cognitive function and activities of living in stroke patients. J. Phys. Ther. Sci. 2015, 27, 2487–2489. [Google Scholar] [CrossRef] [Green Version]
- Cho, H.; Kim, K.; Jung, J. Effects of neurofeedback and computer-assisted cognitive rehabilitation on relative brain wave ratios and activities of daily living of stroke patients: A randomized control trial. J. Phys. Ther. Sci. 2016, 28, 2154–2158. [Google Scholar] [CrossRef] [Green Version]
- Jiang, C.; Yang, S.; Tao, J.; Huang, J.; Li, Y.; Ye, H.; Chen, S.; Hong, W.; Chen, L. Clinical Efficacy of Acupuncture Treatment in Combination with RehaCom Cognitive Training for Improving Cognitive Function in Stroke: A 2 × 2 Factorial Design Randomized Controlled Trial. J. Post Acute Long Term Care Med. 2016, 17, 1114–1122. [Google Scholar] [CrossRef] [Green Version]
- Donnan, G.A.; Fisher, M.; Macleod, M.; Davis, S.M. Stroke. Lancet 2008, 371, 1612–1623. [Google Scholar] [CrossRef]
- Eriksson, M.; Dahlin-Ivanoff, S. How Adults with Acquired Brain Damage Perceive Computer Training as a Rehabilitation Tool: A Focus-group Study. Scand. J. Occup. Ther. 2002, 9, 119–129. [Google Scholar] [CrossRef]
- Jung, H.; Daneault, J.; Lee, H.; Kim, K.; Kim, B.; Park, S.; Ryu, T.; Kim, Y.; Lee, S.I. Remote Assessment of Cognitive Impairment Level based on Serious Mobile Game Performance: An Initial Proof of Concept. IEEE J. Biomed. Health Inform. 2019, 23, 1269–1277. [Google Scholar] [CrossRef]
- Chun, M.M.; Turk-Browne, N.B. Interactions between Attention and Memory. Curr. Opin. Neurobiol. 2007, 17, 177–184. [Google Scholar] [CrossRef]
- Strub, R.L.; Black, F.W. The Mental Status Examination in Neurology; F. A. Davis Company: Philadelphia, PA, USA, 2000. [Google Scholar]
- Squire, L.R. Memory and Brain; Oxford University Press: New York, NY, USA, 1987. [Google Scholar]
- Downing, P.E. Interactions Between Visual Working Memory and Selective Attention. Curr. Opin. Neurobiol. 2000, 11, 467–473. [Google Scholar] [CrossRef]
- Kang, Y.; Na, D.L.; Hahn, S. A validity study on the Korean Mini-Mental State Examination (K-MMSE) in dementia patients. J. Korean Neurol. Assoc. 1997, 15, 300–308. [Google Scholar]
- Miyamoto, S.; Kondo, T.; Suzukamo, Y.; Michimata, A.; Izumi, S. Reliability and Validity of the Manual Function Test in Patients with Stroke. Am. J. Phys. Med. Rehabil. 2009, 88, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Tombaugh, T.N.; McIntyre, N.J. The mini-mental state examination: A comprehensive review. J. Am. Geriatr. Soc. 1992, 40, 922–935. [Google Scholar] [CrossRef] [PubMed]
- Tombaugh, T.N. Test-retest reliable coefficients and 5-year change scores for the MMSE and 3MS. Arch. Clin. Neuropsychol. 2005, 20, 485–503. [Google Scholar] [CrossRef] [Green Version]
- Weiss, L.G.; Saklofske, D.H.; Coalson, D.; Raiford, S.E. WAIS-IV Clinical Use and Interpretation: Scientist-Practitioner Perspectives; Academic Press: New York, NY, USA, 2010. [Google Scholar]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A “quick and dirty” usability scale. In Usability Evaluation in Industry; Jordan, P.W., Thomas, B., McClelland, I.L., Eds.; Taylor & Francis: London, UK, 1996; pp. 189–194. [Google Scholar]
- Bangor, A.; Kortum, P.; Miller, J. Determining what individual SUS scores mean: Adding an adjective rating scale. J. Usability Stud. 2009, 4, 114–123. [Google Scholar]
- Hensel, A.; Angermeyer, M.C.; Riedel-Heller, S.G. Measuring cognitive change in older adults: Reliable change indices for the Mini-Mental State Examination. J. Neurol. Neurosurg. Psychiatry 2007, 78, 1298–1303. [Google Scholar] [CrossRef]
- De Paula, J.J.; Malloy-Diniz, L.F.; Romano-Silva, M.A. Reliability of working memory assessment in neurocognitive disorders: A study of the Digit Span and Corsi Block-Tapping tasks. Braz. J. Psychiatry 2016, 38, 262–263. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.L.; Hsieh, C.L.; Wu, R.M.; Lu, W.S. Test-retest reliability and minimal detectable change of the Beck Depression Inventory and the Taiwan Geriatric Depression Scale in patients with Parkinson’s disease. PLoS ONE 2017, 12, e0184823. [Google Scholar] [CrossRef] [Green Version]
- Zucchell, C.; Capone, A.; Codella, V.; Vecchione, C.; Buccino, G.; Sandrini, G.; Pierelli, F.; Bartolo, M. Assessing and restoring cognitive functions early after stroke. Neuropsychol. Rev. 2014, 29, 255–263. [Google Scholar] [CrossRef]
- Prokopenko, S.V.; Mozheyko, E.Y.; Petrova, M.M.; Koryagina, T.D.; Kaskaeva, D.S.; Chernykh, T.V.; Shvetzova, I.N.; Bezdenezhnih, A.F. Correction of poststroke cognitive impairments using computer programs. J. Neurol. Sci. 2013, 325, 148–153. [Google Scholar] [PubMed]
- Kim, B.R.; Chun, M.H.; Kim, L.S.; Park, J.Y. Effect of Virtual Reality on Cognition in Stroke Patients. Ann. Rehabil. Med. 2011, 35, 450–459. [Google Scholar] [PubMed] [Green Version]
- Sturm, W.; Willmes, K. Efficacy of a reaction training on various attentional and cognitive functions in stroke patients. Neuropsychol. Rehabil. 1991, 1, 259–280. [Google Scholar]
- Ȧkerlund, E.; Esbjörnsson, E.; Sunnerhagen, K.S.; Björkdahl, A. Can computerized working memory training improve impaired working memory, cognition and psychological health? Brain Inj. 2013, 27, 1649–1657. [Google Scholar]
- Choi, D.J.; Lee, D.Y.; Seo, E.H.; Jo, M.K.; Sohn, B.K.; Choe, Y.M.; Byun, M.S.; Kim, J.W.; Kim, S.G.; Yoon, J.C.; et al. A Normative Study of the Digit Span in an Educationally Diverse Elderly Population. Psychiatry Investig. 2014, 11, 39–43. [Google Scholar]
- Patel, S.; Park, H.; Bonato, P.; Chan, L.; Rodgers, M. A review of wearable sensors and systems with application in rehabilitation. J. Neuroeng. Rehabil. 2012, 9, 21. [Google Scholar]
- Beursgens, L.; Boesten, F.; Timmermans, A.; Seelen, H.; Markopoulos, P. Us’Em: Motivating Stroke Survivors to Use Their Impaired Arm and Hand in Daily Life. In CHI ’11 Extended Abstracts on Human Factors in Computing Systems; ACM: New York, NY, USA, 2011; pp. 1279–1284. [Google Scholar]
- Jamieson, M.; O’Neill, B.; Cullen, B.; Lennon, M.; Brewster, S.; Evans, J. ForgetMeNot: Active Reminder Entry Support for Adults with Acquired Brain Injury. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems, Denver, CO, USA, 6–11 May 2017; ACM: New York, NY, USA, 2017; pp. 6012–6023. [Google Scholar] [CrossRef] [Green Version]
- Ben-Sadoun, G.; Sacco, G.; Manera, V.; Bourgeois, J.; König, A.; Foulon, P.; Fosty, B.; Bremond, F.; d’Arripe Longueville, F.; Robert, P. Physical and cognitive stimulation using an exergame in subjects with normal aging, mild and moderate cognitive impairment. J. Alzheimer Dis. 2016, 53, 1299–1314. [Google Scholar]
- Mawson, S.; Nasr, N.; Parker, J.; Davies, R.; Zheng, H.; Mountain, G. A personalized self-management rehabilitation system with an intelligent shoe for stroke survivors: A realist evaluation. JMIR Rehabil. Assist. Technol. 2016, 3, e1. [Google Scholar]
- Choe, E.K.; Lee, B.; Andersen, T.O.; Wilcox, L.; Fitzpatrick, G. Harnessing the power of patient-generated data. IEEE Pervasive Comput. 2018, 17, 50–56. [Google Scholar]
- Parker, J.; Mawson, S.; Mountain, G.; Nasr, N.; Davies, R.; Zheng, H. The provision of feedback through computer-based technology to promote self-managed post-stroke rehabilitation in the home. Disabil. Rehabil. Assist. Technol. 2014, 9, 529–538. [Google Scholar]
- Gulotta, R.; Forlizzi, J.; Yang, R.; Newman, M.W. Fostering engagement with personal informatics systems. In Proceedings of the 2016 ACM Conference on Designing Interactive Systems, Brisbane, Australia, 4–8 June 2016; pp. 286–300. [Google Scholar]
- Hosking, S.; Marsh, N.; Friedman, P. Depression at 3-months poststroke in the elderly: Predictors and indicators. Int. J. Rehabil. Res. 2000, 7, 205–216. [Google Scholar]
- Ayerbe, L.; Ayis, S.; Crichton, S.; Wolfe, C.; Rudd, A. The natural history of depression up to 15 years after stroke: The South London Stroke Register. Stroke 2013, 44, 1105–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, A.; Sun, Q.; Okereke, O.; Rexrode, K.; Hu, F. Depression and risk of stroke morbidity and mortality: A meta-analysis and systematic review. J. Am. Med Assoc. (JAMA) 2011, 306, 1241–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturm, J.; Donnan, G.; Dewey, H.; Macdonnell, R.; Gilligan, A.; Srikanth, V.; Thrift, A. Quality of life after stroke: The North East Melbourne Stroke Incidence Study (NEMESIS). Stroke 2004, 35, 2340–2345. [Google Scholar] [CrossRef] [Green Version]



| Baseline Demographic Data for 29 Stroke Survivors | Experimental | Control |
|---|---|---|
| Patients, No. | 14 | 15 |
| Age, mean (standard deviation), y. | 72.71 (9.86) | 72.67 (12.64) |
| Sex, No. (%) | ||
| Men | 2 (14.29) | 2 (13.33) |
| Women | 12 (85.71) | 13 (86.67) |
| Diagnosis, No. (%) | ||
| Ischemic stroke | 11 (78.57) | 13 (86.67) |
| Hemorrhagic stroke | 3 (21.43) | 2 (13.33) |
| Chronicity, mean (standard deviation), m. | 74.07 (40.84) | 45.47 (19.82) * |
| Affected Side, No. (%) | ||
| Left | 7 (50.00) | 5 (35.71) |
| Right | 7 (50.00) | 9 (64.29) |
| Manual Function test, mean (standard deviation) score | ||
| Affected Limb | 14.00 (9.65) | 15.80 (6.60) |
| Unaffected Limb | 27.07 (2.37) | 28.33 (1.91) |
| MMSE, mean (standard deviation) score | ||
| Orientation | 7.93 (1.82) | 8.07 (1.49) |
| Register | 2.57 (0.51) | 2.13 (0.83) |
| Attention and calculation | 2.57 (0.51) | 2.13 (0.83) |
| Recall | 1.21 (0.80) | 0.67 (0.62) |
| Language | 7.71 (0.83) | 7.87 (0.63) |
| Total score | 21.64 (1.08) | 20.87 (1.30) |
| Digit spanning, mean (standard deviation) score | ||
| Forward | 7.36 (2.17) | 6.13 (1.25) |
| Backward | 4.14 (1.29) | 2.93 (0.88) |
| GDS, mean (standard deviation), score | 3.79 (0.43) | 4.00 (0.00) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, H.-T.; Daneault, J.-F.; Nanglo, T.; Lee, H.; Kim, B.; Kim, Y.; Lee, S.I. Effectiveness of a Serious Game for Cognitive Training in Chronic Stroke Survivors with Mild-to-Moderate Cognitive Impairment: A Pilot Randomized Controlled Trial. Appl. Sci. 2020, 10, 6703. https://doi.org/10.3390/app10196703
Jung H-T, Daneault J-F, Nanglo T, Lee H, Kim B, Kim Y, Lee SI. Effectiveness of a Serious Game for Cognitive Training in Chronic Stroke Survivors with Mild-to-Moderate Cognitive Impairment: A Pilot Randomized Controlled Trial. Applied Sciences. 2020; 10(19):6703. https://doi.org/10.3390/app10196703
Chicago/Turabian StyleJung, Hee-Tae, Jean-Francois Daneault, Tenzin Nanglo, Hyunsuk Lee, Byeongil Kim, Yangsoo Kim, and Sunghoon Ivan Lee. 2020. "Effectiveness of a Serious Game for Cognitive Training in Chronic Stroke Survivors with Mild-to-Moderate Cognitive Impairment: A Pilot Randomized Controlled Trial" Applied Sciences 10, no. 19: 6703. https://doi.org/10.3390/app10196703