






Fact Sheet: Fetal Survival and Risk of Pregnancy Loss


To view this fact sheet as a PDF see: Fact Sheet: Fetal Survival and Risk of Pregnancy Loss
Last updated July 2021
Maternal measures that help reduce the risk of fetal disease
With advancements in science, non-surgical interventions are available to women that can increase pregnancy health. A mother’s daily consumption of folic acid and immunization are important proactive steps that every mother can take to decrease the risk of disease for herself and her baby.
Folic acid consumption:
Perhaps the best-known and most extensively studied prenatal intervention is maternal consumption of folic acid (Vitamin B9) in her diet prior to conception and during pregnancy for reducing the risk of serious birth defects of the baby’s brain (also known as neural tube defects). The two most common types of neural tube defects are anencephaly and spina bifida. Anencephaly is a serious birth defect in which parts of a baby’s brain and skull do not form correctly. There is no known cure for anencephaly. Spina bifida is another serious birth defect in which a baby’s spine does not develop correctly. Babies with the most severe form called myelomeningocele may have severe neurologic and intellectual impairment, including paralysis.
Folic acid has been proven to reduce the incidence of neural tube defects in women with one or more previously affected children and in women who have no risk factors.[1] For this reason, the CDC urges all women of reproductive age who might become pregnant to consume 400 mcg of folic acid every day, in addition to consuming food with folate from a well-balanced diet.[2]
Since starting mandatory folic acid fortification of cereal grain products in the United States in 1998, more babies have been born healthy. A key study from 2015 found that the proportion of babies in the population born with a neural tube defect has decreased by 35% in the United States resulting in about 1,300 more babies born healthy without a neural tube defect each year because of mandatory fortification.[3]
Maternal immunization:
Vaccines administered during pregnancy can provide protection for the mother and baby against serious infectious diseases. Maternal immunization boosts the concentration of maternal antibodies, which can transfer across the placenta to the baby, providing protection until the infant is old enough to be immunized after birth.[4] Maternal immunization can also provide indirect protection, achieved through prevention of maternal infection and through breast milk antibodies.[5]
Vaccination for influenza (the flu) is recommended for all pregnant women to reduce the risk of severe illness caused by the influenza virus, which could be fatal.[6] A 2018 study found that vaccination reduced a pregnant woman’s risk of being hospitalized with the flu by an average of 40 percent.[7] Despite the fact that the influenza vaccine is safe and reduces risk for mom and baby, about ½ of pregnant women still do not get vaccinated.[8]
Early heartbeat detection is a prognostic indicator of fetal survival
Numerous published studies document that detection of a fetal heartbeat, verification of a live embryo or fetus, is a prognostic indicator for survival of the fetus to term. Even early detection of fetal heartbeat points to long-term survival. For example, Seungdamrong et al. found that ultrasound detection of fetal cardiac activity at 6 weeks’ gestation had a 93% positive predictive value for successful completion of the first trimester in IVF pregnancies.[9] Bae and Karnitis found that detection of fetal cardiac activity at 7 weeks’ gestation had a 90.5% predictive value for fetal survival and ongoing pregnancy.[10]
Hyer et al. showed that presence of a heartbeat at 6-8 weeks’ gestation correlated with a live birth rate of 98% in normal pregnancies without intervention.[11] Doubilet et al., showed that ultrasound detection of a normal heartbeat at 7 weeks‘ gestation predicted 91.5% survival to the end of the first trimester, and those survivors proceeded at a rate of 95.1% to be liveborn infants.[12] Cashner et al. published similar findings that, if a live fetus is documented by ultrasonography at 8-12 weeks’ gestation, survival to at least 20 weeks’ gestation is 98.0%.[13]
Likewise MacKenzie et al. found that in the normal population, women with a viable pregnancy at less than 12 weeks’ gestation as detected by ultrasound showed 98% fetal survival up to 28 weeks.[14] The primary determinant associated with a live embryo or fetus was ultrasound detection of a heartbeat.
In utero therapies that increase fetal function and survival
Birth defects are the leading cause of infant deaths, affecting approximately one in every 33 live births (about 3%) in the United States each year and accounting for 20% of all infant deaths.[15],[16]Environmental risk factors have been identified that contribute to neural tube defects, including the lack of folic acid supplementation and low dietary intake of folate described above. However, there are other genetic and environmental causes that prenatal vitamins alone cannot correct. For some of these birth defects there are fetal treatment options.
Fetal therapy
Fetal therapy is an exciting advancement in maternal-fetal medicine with the goal to repair structural defects before birth and possibly even cure disease in the prenatal period. Such revolutionary advancements in fetal surgery have proven successful for reducing infant mortality in treatment of several conditions including sacrococcygeal teratoma (SCT), congenital diaphragmatic hernia (CDH), congenital cystic adenomatoid malformations (CCAM), severe kidney obstruction and oligohydramnios, spina bifida, twin-to-twin transfusion syndrome (TTTS), and many others.[17] Almost monthly, we hear in the news about another baby who received life-saving fetal surgery using advanced medical techniques. In fact, Children’s Hospital of Philadelphia recently celebrated the birth of their 2,000th fetal surgery patient.[18]
Spina bifida
Significant infant improvements have been observed in myelomeningocele, the most severe form of spina bifida, The Management of Myelomeningocele Study (MOMS) found that fetal surgery on fetuses with spina bifida before 26 weeks’ gestation was associated with a decreased risk of death or shunting before postnatal age 12 months, as well as improved mental and motor function (including independent walking) at 30 months of age.[19] Researchers in the follow-up MOMS2 trial have shown those benefits continue into childhood, up to 10 years after birth.[20]
Twin-to-twin transfusion syndrome
In another example, minimally invasive fetal surgery for treating twin-to-twin transfusion syndrome (TTTS) has saved the lives of one or both twins at all stages of disease between 16-26 weeks’ gestation conventionally, and as early as 14-15 weeks in severe cases.[21] High-volume fetal therapy centers, such as the Children’s Hospital of Philadelphia (CHOP) Center for Fetal Diagnosis and Treatment, report a higher than 90% survival rate of at least one twin and a higher than 80% survival rate of both twins after laser ablation.[22] The Cincinnati Children’s Fetal Center reports similar data of higher than 80% overall survival of at least one or both twins.[23]
Alpha-thalassemia
In utero hematopoietic cell transplantation (IUHCT) is another form of fetal therapy using adult stem cells to treat specific blood disorders and congenital disease that can be diagnosed prenatally. Adult stem cells from a healthy donor, such as the mother or father, are transplanted into the recipient fetus for repair of diseased cells. In patients with alpha-thalassemia major (ATM), a disease resulting in fetal demise and severe neurological impairments, fetal therapy with serial in utero transfusions has shown potential for fetuses surviving to term with normal neurologic outcomes.[24] The world’s first in utero stem cell transplant was performed by Dr. Tippi Mackenzie at UCSF Medical Center, who successfully and safely transplanted a mother’s own stem cells into her unborn fetus diagnosed with alpha-thalassemia.[25]
Risk of early, intermediate, and late pregnancy loss
Early fetal loss is defined as the natural demise of the fetus before 20 weeks completed, also known as a miscarriage. Intermediate loss between 20-27 weeks and late fetal loss of 28 weeks or more is called a stillbirth. The risk of fetal loss is highest during the first trimester (prior to 12 weeks) and decreases beyond 12 weeks’ gestation. More detailed risks by week are given below based on various reports.
- A 2018 study reported that among all self-reported pregnancies, excluding induced terminations, the risk of pregnancy loss was 19.7% and early pregnancy loss was 13.5% during 1990–2011.[26]
- The March of Dimes reports that most miscarriages happen in the first trimester before the 12th week of pregnancy. Miscarriage in the second trimester (between 13 and 19 weeks) happens in 1 to 5 in 100 (1 to 5 percent of) pregnancies.[27]
- Four independent studies report that by week 14, the miscarriage rate falls below 10 miscarriages per 1,000 (<1%) and drops even lower through week 20.[28]
- Risk of fetal loss at 15 weeks is < 1% in both white and black women.[29]
- About 1 pregnancy in 100 (or about 6 per 1,000; <1%) at 20 weeks of pregnancy and later is affected by stillbirth, and each year about 24,000 babies are stillborn in the United States.[30]
Active treatment in extremely premature increases survival
Babies born extremely premature can receive advanced medical care and active treatment to increase their chances of survival.[31] Such active care is enabling babies to survive younger and younger, as early as 21 weeks’ gestation.
Diana’s Story–”TwentyTwo Matters”
A mom shared her daughter’s journey as the “smallest surviving baby” at an Orlando hospital (22 weeks 4 days, 340 grams). She stated, “Remember this story when someone says a baby is ‘too small to be intubated.’” https://www.facebook.com/groups/273628386593418/permalink/706840789938840/
Story of Jemarius Jachin Harbor
Jemarius Jachin Harbor born at Emory Decatur Hospital in Georgia at only 21 weeks young, weighing only 13 ounces, smaller than the size of a hand on Friday December 20, 2019. The baby had extremely low odds of survival. The mother had lost two previous preemies at 22 weeks each. As she reported to local news station, -quote: “We looked at each other in the eye and I told him [doctor] just give it a try. I just want you to try as long as you try that’s all that matters to me, don’t just up and say that you can’t do it. Just ‘cause you haven’t done it doesn’t mean it can’t be done,” said McPherson. And her little baby boy was treated and survived.[32]
Story of Richard Scott William Hutchinson
Richard Scott William Hutchinson was born at 21 weeks’ gestation in June 2020, during the pandemic shutdown (weighing less than a can of soda) at Children’s Minnesota, who celebrated his first birthday earlier this year. His parents were initially told that he had a 0% chance of survival but then received the advanced care he needed and survived.[33]
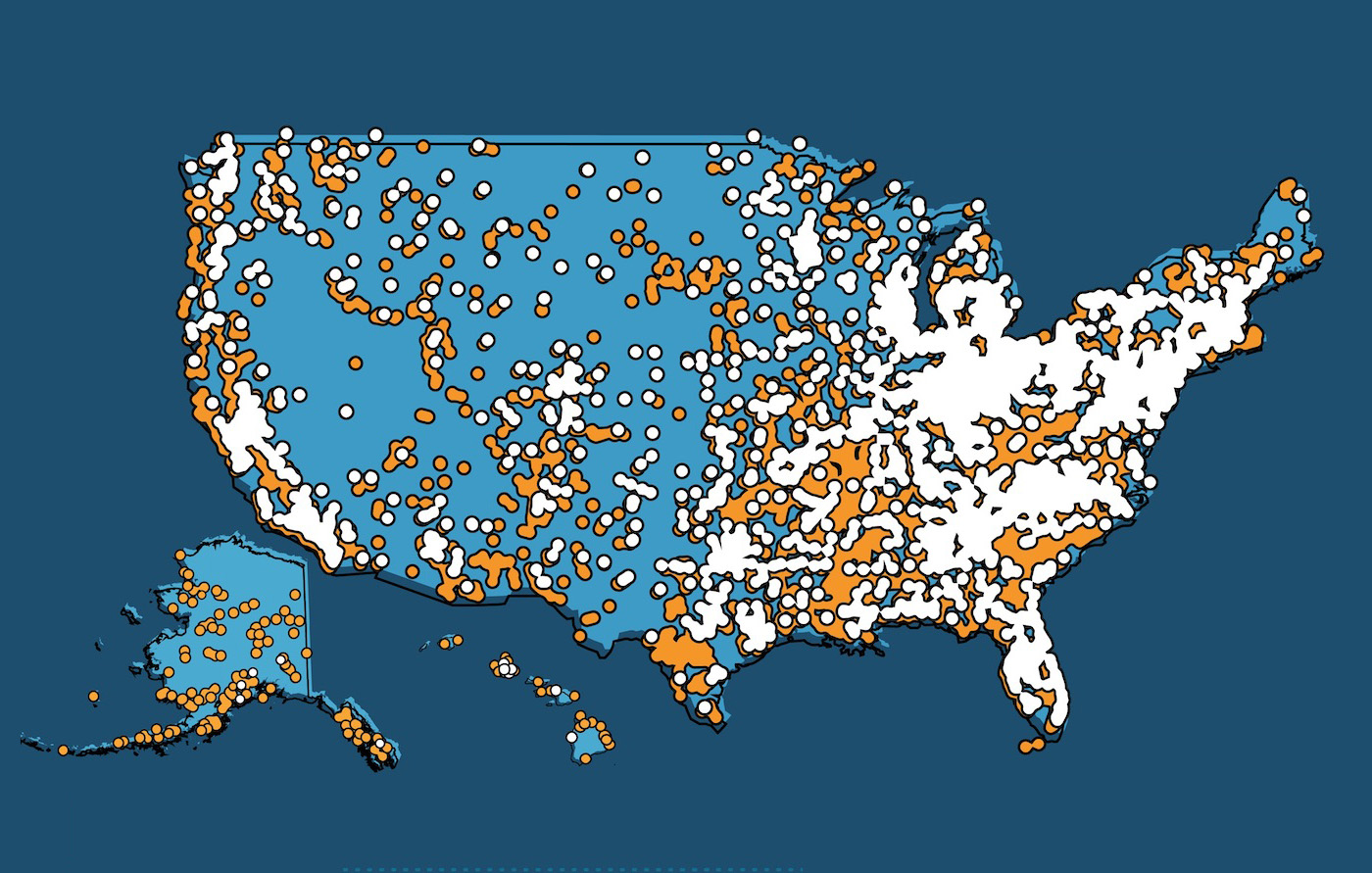
Hospitals equipped to give active treatment to babies at 22 weeks:
22 Weekers Map: These are hospitals that confirmed to have saved a 22 weeker through the parent.
[1] Martinez-Frias, M.L. and E. Rodriguez-Pinilla, Folic acid supplementation and neural tube defects. Lancet, 1992. 340(8819): p. 620.
[2] Centers for Disease Control and Prevention. Folic Acid Helps Prevent Neural Tube Defects
Available at: https://www.cdc.gov/ncbddd/folicacid/data.html
[3] Williams J, Mai CT, Mulinare J, et al. Updated estimates of neural tube defects prevented by mandatory folic acid fortification – United States, 1995–2011. MMWR Morb Mortal Wkly Rep. 2015;64(1):1–5
[4] Munoz FM, Jamieson DJ. Maternal Immunization. Obstet Gynecol. 2019 Apr;133(4):739-753. doi: 10.1097/AOG.0000000000003161. PMID: 30913173.
[5] ibid
[6] Centers for Disease Control and Prevention. Flu & Pregnant Women. Available at: https://www.cdc.gov/flu/highrisk/pregnant.htm
[7] Mark G Thompson, Jeffrey C Kwong, Annette K Regan, Mark A Katz, Steven J Drews, Eduardo Azziz-Baumgartner, Nicola P Klein, Hannah Chung, Paul V Effler, Becca S Feldman, Kimberley Simmonds, Brandy E Wyant, Fatimah S Dawood, Michael L Jackson, Deshayne B Fell, Avram Levy, Noam Barda, Lawrence W Svenson, Rebecca V Fink, Sarah W Ball, Allison Naleway, Influenza Vaccine Effectiveness in Preventing Influenza-associated Hospitalizations During Pregnancy: A Multi-country Retrospective Test Negative Design Study, 2010–2016, Clinical Infectious Diseases, Volume 68, Issue 9, 1 May 2019, Pages 1444–1453, https://doi.org/10.1093/cid/ciy737
[8] Centers for Disease Control and Prevention. Maternal Immunization: Current Status and Future Directions. Available at: https://www.cdc.gov/grand-rounds/pp/2019/20190918-maternal-immunization.html
[9] Seungdamrong A et al., Fetal cardiac activity at 4 weeks after in vitro fertilization predicts successful completion of the first trimester of pregnancy, Fertil Steril 90, 1711, 2008; doi:10.1016/j.fertnstert.2007.08.018
[10] Bae S and Karnitis J, Triple ultrasound markers including fetal cardiac activity are related to miscarriage risk, Fertility and Sterility 96, 1146, 2011; doi: 10.1016/j.fertnstert.2011.08.009
[11] Hyer JS et al., Predictive value of the presence of an embryonic heartbeat for live birth: Comparison of women with and without recurrent pregnancy loss, Fertility and Sterility 82, 1369, 2004; doi: 10.1016/j.fertnstert.2004.03.058
[12] Doubilet PM et al., Long-Term Prognosis of Pregnancies Complicated by Slow Embryonic Heart Rates in the Early First Trimester, J Ultrasound in Medicine 18, 537, 1999; doi: 10.7863/jum.1999.18.8.537
[13] Cashner KA et al., Spontaneous Fetal Loss After Demonstration of a Live Fetus in the First Trimester, Obstet Gynecol 70, 827, 1987
[14] Mackenzie WE et al., Spontaneous abortion rate in ultrasonographically viable pregnancies, Obstet Gynecol 71, 81, 1988
[15] Centers for Disease Control and Prevention, Data and Statistics on Birth Defects. Available at: https://www.cdc.gov/ncbddd/birthdefects/data.html [Accessed June 10, 2020].
[16] Egbe AC. Birth defects in the newborn population: race and ethnicity. Pediatr Neonatol. 2015;56(3):183‐188. doi:10.1016/j.pedneo.2014.10.002
[17] C. Malloy, M. C. Wubbenhorst, T. Sander Lee, The Perinatal Revolution. Issues in Law and Medicine 34 (1), 15-41 (2019).
[18] Children’s Hospital of Philadelphia Celebrates Birth of 2,000th Fetal Surgery Patient | Children’s Hospital of Philadelphia (chop.edu)
[19] Adzick, N.S., et al., A randomized trial of prenatal versus postnatal repair of myelomeningocele. N Engl J Med, 2011. 364(11): p. 993-1004
[20] Houtrow AJ, Thom EA, Fletcher JM, et al. Prenatal Repair of Myelomeningocele and School-age Functional Outcomes. Pediatrics. 2020;145(2):e20191544. doi:10.1542/peds.2019-1544
[21] Baud D, Windrim R, Keunen J, Kelly EN, Shah P, van Mieghem T, Seaward PG, Ryan G. Fetoscopic laser therapy for twin-twin transfusion syndrome before 17 and after 26 weeks’ gestation. Am J Obstet Gynecol. 2013 Mar;208(3):197.e1-7. doi: 10.1016/j.ajog.2012.11.027. Epub 2012 Nov 21. PMID: 23178244. AND Lecointre L, Sananes N, Weingertner AS, Kohler M, Guerra F, Fritz G, Viville B, Langer B, Nisand I, Favre R. Fetoscopic laser coagulation for twin-twin transfusion syndrome before 17 weeks’ gestation: laser data, complications and neonatal outcome. Ultrasound Obstet Gynecol. 2014 Sep;44(3):299-303. doi: 10.1002/uog.13375. PMID: 24677292.
[22] Children’s Hospital of Philadelphia,”Volumes and Outcomes: Fetal Anomalies.” Available at: https://www.chop.edu/centers-programs/center-fetal-diagnosis-and-treatment/volumes-outcomes
[23] Cincinatti Children’s, ”Twin-twin transfusion syndrome (TTTS).“ Available at: https://www.cincinnatichildrens.org/health/t/twin-twin-transfusion-syndrome
[24] Kreger, E.M., et al., Favorable outcomes after in utero transfusion in fetuses with alpha thalassemia major: a case series and review of the literature. Prenat Diagn, 2016. 36(13): p. 1242-1249.
[25] Suzanne Leigh. Baby Born in World’s First In Utero Stem Cell Transplant Trial. Available at: https://www.ucsf.edu/news/2018/05/410436/baby-born-worlds-first-utero-stem-cell-transplant-trial
[26] Rossen LM, Ahrens KA, Branum AM. Trends in Risk of Pregnancy Loss Among US Women, 1990-2011. Paediatr Perinat Epidemiol. 2018;32(1):19-29. doi:10.1111/ppe.12417
[27] Miscarriage (marchofdimes.org)
[28] Ammon Avalos L, Galindo C, Li DK. A systematic review to calculate background miscarriage rates using life table analysis. Birth Defects Res A Clin Mol Teratol. 2012 Jun;94(6):417-23. doi: 10.1002/bdra.23014. Epub 2012 Apr 18. PMID: 22511535.
[29] Mukherjee S, Velez Edwards DR, Baird DD, Savitz DA, Hartmann KE. Risk of miscarriage among black women and white women in a U.S. Prospective Cohort Study. Am J Epidemiol. 2013;177(11):1271-1278. doi:10.1093/aje/kws393; AND reported in MedicalNewsToday: What are the miscarriage rates per week? Written by Zawn Villines on January 12, 2020. Available at: https://www.medicalnewstoday.com/articles/322634
[30] MacDorman MF, Gregory EC. Fetal and perinatal mortality: United States, 2013. National vital statistics reports: from the Centers for Disease Control and Prevention, National Center for Health Statistics, National Vital Statistics System. 2015; 64(8):1-24; AND the Centers for Disease Control and Prevention. Available at: https://www.cdc.gov/nchs/data/nvsr/nvsr64/nvsr64_08.pdf
[31] Dance A. Survival of the littlest: the long-term impacts of being born extremely early. Nature. 2020 Jun;582(7810):20-23. doi: 10.1038/d41586-020-01517-z. PMID: 32488165; AND Rysavy MA, Li L, Bell EF, Das A, Hintz SR, Stoll BJ, Vohr BR, Carlo WA, Shankaran S, Walsh MC, Tyson JE, Cotten CM, Smith PB, Murray JC, Colaizy TT, Brumbaugh JE, Higgins RD; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Between-hospital variation in treatment and outcomes in extremely preterm infants. N Engl J Med. 2015 May 7;372(19):1801-11. doi: 10.1056/NEJMoa1410689. Erratum in: N Engl J Med. ;372(25):2469. PMID: 25946279; PMCID: PMC4465092; AND Patel RM, Rysavy MA, Bell EF, Tyson JE. Survival of Infants Born at Periviable Gestational Ages. Clin Perinatol. 2017 Jun;44(2):287-303. doi: 10.1016/j.clp.2017.01.009. Epub 2017 Mar 22. PMID: 28477661; PMCID: PMC5424630.
[32] https://www.fox29.com/news/extreme-preemie-born-at-21-weeks-young-at-emory-decatur-hospital
[33] The world’s most premature baby has celebrated his first birthday after beating 0% odds of surviving – CNN












